Changes in body composition – malnutrition, cachexia Determination of resting energy expenditure and nutrition utilization Determination of body composition Comet assay Currently running clinical studies
Changes in body composition – malnutrition, cachexia
Many severe chronic diseases lead to changes in body composition and importance of its accurate determination is still increasing. To the most serious states belongs cachexia, a complex metabolic syndrome associated with underlying illness and characterized by loss of muscle with or without loss of fat mass. The prominent clinical feature of cachexia is weight loss in adults or growth failure in children. Anorexia, inflammation, insulin resistance and increased muscle protein breakdown are frequently associated with wasting disease. It is distinct from starvation, age-related loss of muscle mass, primary depression, malabsorption and hyperthyroidism and is associated with increased morbidity and mortality. The treatment options for cachexia are limited. Unfortunately, refeeding a patient with cachexia does not correct the underlying problem.
Figure 1: Definition of cachexia
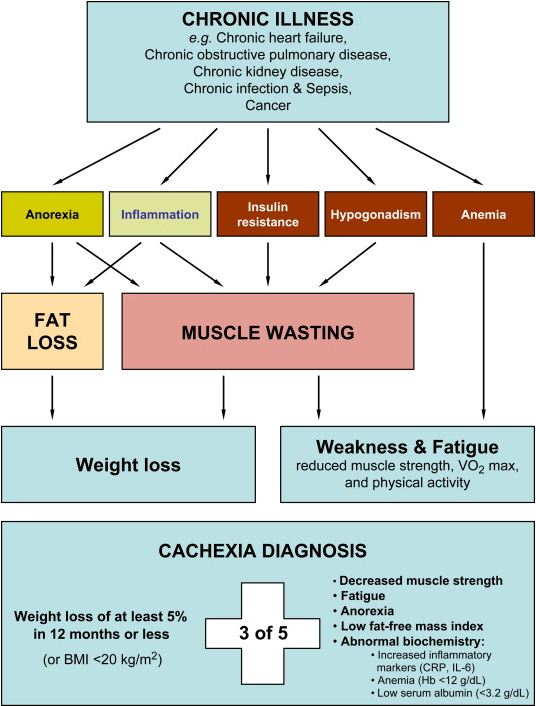
(adapted from Cachexia: a new definition)
Top of page
Determination of resting energy expenditure and nutrition utilization
Resting energy expenditure (REE) represents the amount of calories required for a 24-hour period by the body during a non-active period. The REE is useful to prevent under and overfeeding of individuals, especially in the acute care hospital setting, which can have detrimental effects on clinical outcomes of patients' care. Malnutrition can result from feeding a patient less than his/her metabolic requirements leading to reduced respiratory muscle strength, increased risk of infection, poor wound healing and impaired normal body function. Overfeeding means providing too many calories that cannot be used by the body, and are therefore converted to fat storage. It could result in increased carbon dioxide production and therefore increased work of breathing.
The accepted standard for determining of REE is indirect calorimetry, but it is unavailable or unaffordable in many centers. Indirect calorimetry measures oxygen consumption and carbon dioxide excretion, which are used to calculate the respiratory quotient (ie, the ratio of carbon dioxide excretion to oxygen consumption) and the REE, with the Weir equation. Respiratory quotient is then used to evaluate substrate utilization. In the absence of calorimetry, clinicians use equations (one of the most frequently used formulas for predicted energy expenditure are the Harris-Benedict equations) and clinical judgment to estimate calorie need.
The determination of REE and nutrition utilization by means of indirect calorimetry allows us to estimate both quantitative and qualitative nutrition need of an individual.
Top of page
Determination of body composition
There are many methods to determine body composition, to methods mostly used belong skin-fold anthropometry (SFA), bioelectrical impedance analysis (BIA) and bioimpedance spectroscopy (BIS).
The simplest method of them is SFA which is based on determination of skin folds width. The amount of the subcutaneous fat is determined according to measurement of 3-11 skin folds. The total fat and non-fat tissue could be then estimated by use of specific equation e.g. Durnin and Womersley and/or Siri.
Bioelectrical impedance is non-invasive method based on measurement of bioelectric characteristics of human body. It determines the resistance and reactance on the passage of alternating current of low intensity. BIA is based on measurement at only one present frequency, BIS at whole specter of frequencies. At low frequency, the current does not penetrate the cell membrane and therefore the current passes through the extracellular fluid. At very high frequency the current passes through both intracellular and extracellular fluid. Bioelectrical impedance could be measured at single frequency, generally at 50 kHz (BIA) or by whole spectrum of frequencies (BIS). The body composition is estimated according to specific regression equation acquired by study of homogenous groups of people.
Recently, dual energy X-ray absorptiometry (DEXA) has been suggested as a suitable clinical reference (“gold standard”) method for the measurement of body composition. However DEXA is the most expensive routine method and not common equipment in many hospitals and outpatients' departments.
We used all of above mentioned methods to determine body composition in our research.
Figure 2: Application of high frequency of BIS for measurement of amount intracellular fluid
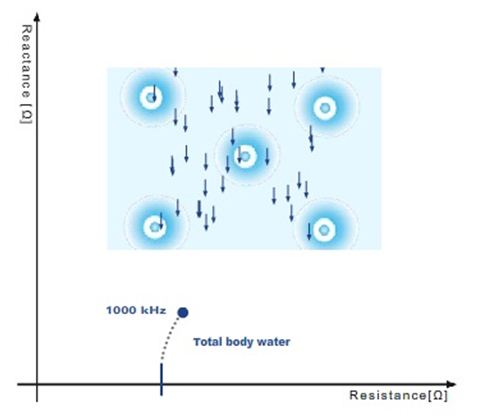
(adapted from Fresenius)
Figure 3: Application of low frequency of BIS for measurement of amount extracellular fluid
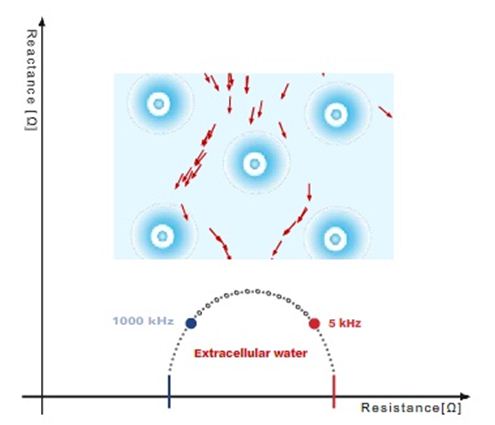
(adapted from Fresenius)
Recently, dual energy X-ray absorptiometry (DEXA) has been suggested as a suitable clinical reference (“gold standard”) method for the measurement of body composition. However DEXA is the most expensive routine method and not common equipment in many hospitals and outpatients' departments.
All of above mentioned methods to determine body composition are used in our research.
Top of page
Comet assay
The comet assay or single-cell gel electrophoresis (SCGE) assay is a rapid, sensitive and relatively simple method for detecting DNA damage at the level of individual cells. This assay is now widely accepted as a standard method for assessing DNA damage in individual cells; it is used in a broad variety of applications including human biomonitoring, genotoxicology, ecological monitoring and as a tool to investigate DNA damage and repair in different cell types in response to a range of DNA-damaging agents. The name comet comes from the similarity of the image obtained in this method to that of the astronomical body, the head consisting of intact DNA and a tail containing damaged and broken pieces of DNA. This shape is created by the electrophoresis, when the DNA migrates out of the cell. The distribution of DNA within the comet correlates with the extent of DNA damage. The comet assay would be eminently suitable for use in clinical practice since it is a relatively simple and inexpensive technique which requires only a few cells, and results can be obtained within a matter of hours. However, despite these advantages, it has not been widely employed as a standard analytical tool within clinical laboratories, partly because there is still some doubt about its reliability, reproducibility and validity. This method can also be modified to measure the DNA repair activity of cell extracts on gel-embedded DNA substrate which harbours specific lesions. Prof. Andrew Collins and his co-workers first designed this kind of experiment to measure the capacity of human lymphocyte extract for site-specific incision, which is the initial step in DNA repair of oxidized bases. Another modification of this method is the so-called Comet-FISH which is a useful tool for detection of region-specific DNA damage. Comet-FISH combines two well-established methods, the Comet assay with fluorescence in situ hybridization (FISH). It is employed in diff erent kinds of probes to clarify the connection in the etiology of diff erent cancers to DNA susceptibility. Some working group use FISH for detection of chromosomal loci associated with cancer and it is also possible to study the kinetics of a specific gene repair involved in cancer. The comet assay has been applied in a broad range of scientific fields, including genetic toxicology, ecotoxicology and DNA repair research.
This assay could be used for determination of DNA damage and repaire, DNA oxidation damage, DNA fragmentation in sperm cells, sensitivity of cancer cells for radio- and chemotherapy or in genotoxicological and chemo-preventive studies.
Figure 4: Fluorescence microscopy visualization of comet assay
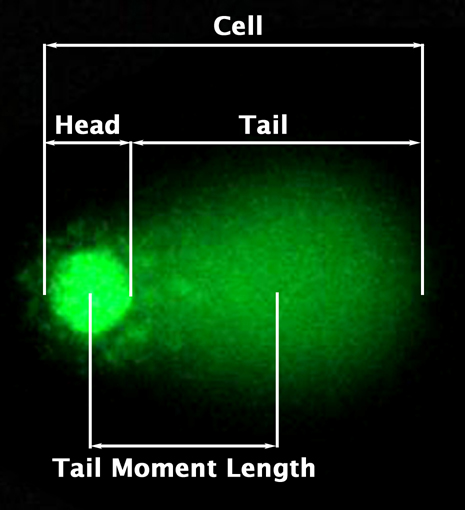
(adapted from cellbiolabs)
Top of page